Archive for the ‘Happy Trails’ Category
Beyond Bypass Surgery
I had bypass surgery in April 2016, a few months before my 69th birthday. In the hospital, they used the acronym “CABG” (pronounced “cabbage”, like the common vegetable), meaning Coronary Artery Bypass Graft. I had gone into the hospital following an – of course – unexpected heart attack, and a cardiac catheter inserted through the wrist a day later had found two arteries 90% blocked and one artery 100% blocked. Stents were ruled out, and I was scheduled for a triple bypass. Receiving the news, I decided to relax as much as possible and just do it – patiently go through the process. I really did not have another choice; the alternative would be a far more serious and possibly terminal heart attack before long. My triple bypass became a quadruple bypass during surgery.
My wife and children were good soldiers during this ordeal, visiting daily while I waited several days for the surgery, then during the brief pre-op transfer and wait, then in the ICU following surgery, and then in a hospital room for several days. I think they were much more concerned than I was, but the medication I was getting probably limited my anxiety. Even during the recovery stay, while it seemed like I was getting checked, poked, and tested 24/7, I remained as patient as a patient could be. Looking back, it does not seem possible that I spent eleven days in the hospital.
My heart attack had been a minor one, if it’s fair to call it that. I had just finished breakfast and decided to move a metal outdoor table from the garage, where I had painted it the day before, out to the deck. It is a round, steel mesh table, probably weighing 25 to 30 pounds. I did not think to warm up for the exercise – what’s the big deal about moving a table to the deck? – I’ve done it many times. However, this time, once I had carried the table to the deck, I felt light headed and a little dizzy. I leaned on the deck railing, expecting the feeling to go away – but it didn’t. I also felt a tightness in my upper chest, almost in my throat, and in my left arm. I was mentally comparing the feelings I was experiencing to heart attack symptoms I had learned from reading; but I couldn’t be sure what this was. I went into the house and into the bedroom and laid down on the bed for a few minutes. After about ten minutes I was engaged in a conversation with my wife about an unrelated matter, and I was up and about again with no symptoms. I then walked down the driveway, got the mail from the mailbox, and started back up the incline. The same symptoms came back. I went into the house and sat down on the couch in the living room. Another ten minutes passed, and I felt better. I then returned to the deck to clean up some fallen leaves and branches with a leaf rake, and the same symptoms came back for the third time. I went back to the living room couch again. My wife and daughter had been aware of my unusual behavior and looked at me with concern. I said, referring to my symptoms, “I think we should get this checked out”. My wife called the doctor and then called 911, and the rescue service was there asking questions and checking my condition within a few minutes. The EKG in the rescue vehicle looked normal, but they said I should load up on aspirin (4 each of the 81 mg pills) and go to the Emergency Room to have conditions checked there, where the equipment is more sophisticated. The responders offered to take me to the ER if I wanted, or my wife could drive me. I should have accepted the offer of a ride in the rescue vehicle, because my wife was very concerned about driving me, despite my nonchalance. A blood test in the ER revealed an elevated level of traponin, an enzyme released into the blood stream when there is heart damage – another sign of a heart attack. I was then checked into the hospital and scheduled for the cardiac catheter for a close-up look at internal conditions.
My father died about 40 years ago of a heart attack at age 54. He appeared to be physically fit, and he was not overweight. He had one heart attack, a terminal heart attack precipitated by atherosclerosis – commonly known then as hardening of the arteries. He smoked a pack of cigarettes every day, he ate a lot of red meat, and he drank hard liquor – more in the years just before he died. In those later years, he also developed a tremor, and involuntary slight shaking of the hand. His mother (my grandmother) had died a few years earlier of similar conditions at age 73. It seemed to be in the genes.
However, comparing myself to my father and comparing my lifestyle to his, I thought I was free and clear of any heart problems. Although I have never been an athletic person, I enjoy hiking and bicycling; my wife and I take hiking vacations; I do 3-mile walks three or more times every week; we have and use indoor exercise equipment; I did smoke but quit 30 years ago; and our diet has long been quite limited in fat and sodium. I have been taking cholesterol and blood pressure medications for about 20 years and low-dose aspirin for about 10 years. I assumed that my health conscious lifestyle would be sufficient to prevent a heart attack.
Following bypass surgery, I began to remember changes in recent years that might have been hints of what was to come. On hikes taken during the last two years, I had to make more frequent rest stops; I had dismissed that as nothing more than a sign that I was getting old. And, on the first slight uphill stretches on early morning walks during the last year, I had sometimes felt a discomfort in my upper chest – throat area similar to acid reflux; I had dismissed that as a result of drinking morning coffee and not enough water. Cardiac analysis during my hospital stay suggested I had experienced previous, minor damage to heart tissue. So, maybe those incidents had been little cardiac events, and my response to them amounted to denial. For others experiencing similar symptoms, a heart check-up may be informative and may allow for preventive intervention.
Considering it from my current perspective, I think my heart attack was a long time in the making, a gradual, decades long closing down of the arteries that was offset in part by regular exercise that helped to develop collateral circulation in the heart – alternative routes for oxygen rich blood to bypass the developing blockages. While I was waiting the several days for scheduled bypass surgery, one of the doctors referred to my heart attack as “a shot across the bow”. I started thinking of it as a “lucky” heart attack, one that gives you an opportunity to remake your life, to improve an already good diet, to improve and expand on good exercise, and, perhaps most important, to enjoy and appreciate the people and activities that may have been taken for granted a bit too much. I really did see it as a new beginning, and I was really excited to look forward to good prospects and new choices.
During hospital recovery after the surgery, my condition improved daily. I started with short walks in the hallway and gradually longer walks and a stair climb. At first I had to overcome a minor dizziness caused by a post-op medication. Each day saw the removal of one or more tubes and monitor wires, and I was completely disconnected from the medical equipment by the fifth day. The hospital food was surprisingly good, and they monitored my orders to make sure I stayed within cardiac dietary restrictions. It was also quite helpful that my son brought me a large cup of good coffee from outside the hospital each morning.
Following my discharge from the hospital, the first phase of recovery at home brought a new routine. Logging of daily medications, weight, blood pressure, and temperature were part of the routine. Morning and afternoon naps were also part of the routine for a few weeks, followed by less frequent afternoon naps before naps were forgotten. Pillows took on an important role. I had to sleep on my side with a pillow behind me and another between my knees. If I went anywhere in a car, I had to ride in the back seat with a pillow between my chest and the shoulder strap of the seat belt. The requirement for the chest pillow and use of the back seat were to help minimize possible harm to my healing chest incision (sternotomy). My wife was able to make arrangements to work from home for several weeks so that she could help with my recovery, and, during the six weeks before my follow-up appointment with the surgeon, she would drive and had to tolerate my backseat driver behavior. She also studied the cardiac dietary guidelines and found ways to reduce the fat and sodium in our already lean eating habits. We resumed our daily outside walks, very limited in distance for the first few days but increasing in length to our previous 3-mile walking distance within about 3 weeks of returning home. A visiting nurse had been authorized for one visit per week, but that was discontinued after two visits. Part of the recovery criteria is a lifting limit of ten pounds for the first six to twelve weeks; I gladly left most lifting to others during the first six weeks; in a post surgery follow-up appointment after about six weeks, the surgeon increased the limit to thirty pounds and also said I could start driving again. During the first two weeks after discharge from the hospital, I used an incentive spirometer (photo below) several times each day for to help increase my lung capacity, raising the target several times as my lung capacity increased.

Airlife incentive spirometer
There have been a few changes in prescribed medication following my bypass surgery. A metoprolol beta blocker that was started before surgery was discontinued soon after discharge, and an ACE inhibitor (lisinopril) was discontinued in favor of losartan, which I had used previously for many years. The ACE inhibitor was thought to have caused a persistent cough that developed soon after surgery, and the change back to losartan – a different type of blood pressure medication – was successful in eliminating the cough. Another change of significance (I think) related to the bypass surgery was a change from a generic simvastatin (a cholesterol medication I had taken during the several years since a patent expired for Lipitor and insurance companies refused to pay for it any longer) to atorvastatin (another name for lipitor); a blood test following the change to atorvastatin showed strikingly lower cholesterol levels compared with results from a test a few months earlier when I was taking simvastatin. There was also a change in non-prescribed medication: I stopped taking glucosamine, which I had started taking six years ago to help overcome joint stiffness I had mistakenly attributed to arthritis or just getting older. After the bypass surgery, I decided to try life without the glucosamine, and I have now found that I don’t miss it; my joints are not stiff.
My weight also changed following surgery. When I left the hospital, I weighed about ten pounds less than I had weighed when I went into the hospital; then I lost another five pounds (probably from retained water) during my first week at home. Since then, during recovery and monitored cardiac rehabilitation, I have lost another five pounds, so that I am now about twenty pounds lighter than I was when I went into the hospital. My goal is to lose another ten pounds over several months. I have tried a few different weight loss diets (Weight Watchers, South Beach, etc.) over the years; this time I plan to simply continue a balanced diet, managing intake (based on healthy dietary targets for calories, fats, and sodium) and output (calories burned through exercise) to realize a gradual loss of weight to reach my goal and then maintain the lower weight, which will also be within my recommended BMI range. If I accomplish that, I will then be maintaining a low weight level I have not seen for nearly forty years – a worthy goal for many of us.
Now, it seems that getting older was just a myth I had used to explain away symptoms, and, for the short term at least, it is a thing of the past. With improved circulation and improving fitness from the monitored cardiac rehab exercise program, I feel much younger than I can remember feeling for the last twenty or more years, and my bucket list is getting longer. But there is more.
Considering family members, I think it’s important to make recovery and rehab choices for the benefit of those who were so affected and concerned and who hung in there for me and provided so much support during my hospital stay and subsequent recovery. I recently completed a mandatory twelve week monitored cardiac rehab program, and I now need to continue with a self-managed exercise program to maintain a good level of cardiac fitness. I understand that many who start the monitored program do not complete it, and many who participate in the program soon fall back into their old ways, bringing on another cardiac event before much time has passed. I don’t want to let that happen. I want to avoid it for my own benefit, but, more than that, I want to remain healthy for a long time for the benefit of my family. I see them differently now than I did before my heart attack, and I see myself differently. So, I am now looking for improved self-discipline to serve these purposes. I want to be fit to see many new sunrises, and I want to share those with the people I love.

another sunrise
Taking the Hump
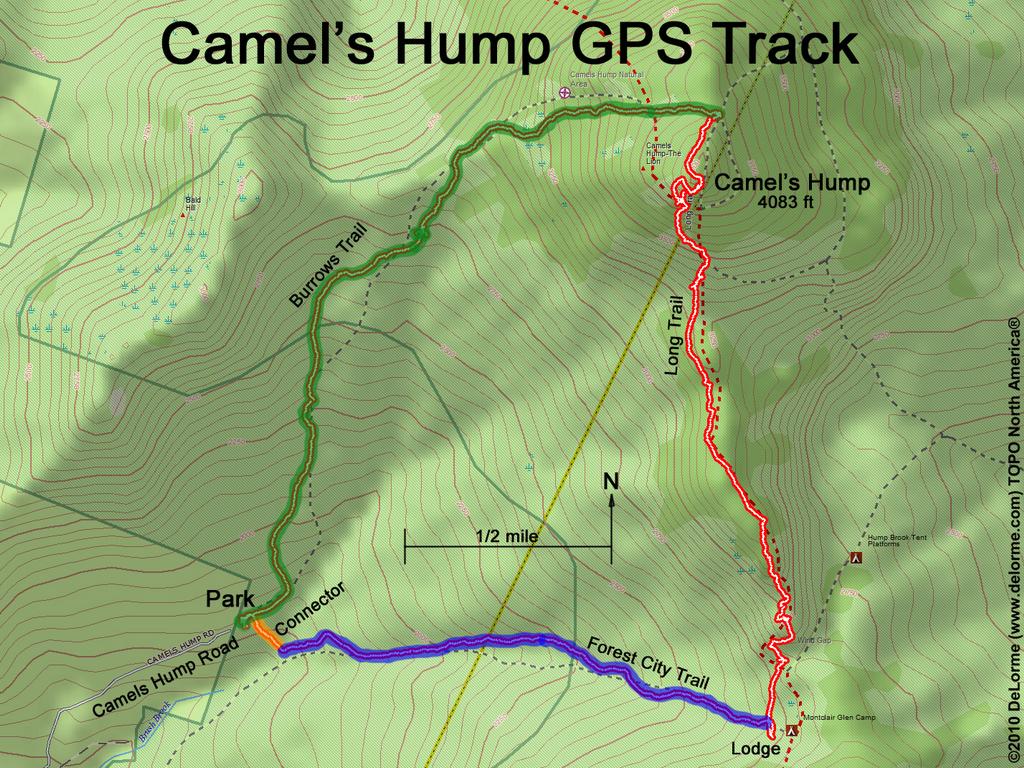
In August 2015, after a little more than 25 years in northwestern Vermont, including an increasing amount of hiking in the last few years – though mostly on vacations in the western U.S., my wife and I decided it was time to hike to the top of Camel’s Hump. We had hiked a few of the less famous mountains in Vermont and had mistakenly concluded that the rocky trails we encountered at Worcester Mountain and Elmore Mountain were unusual and not the norm to be expected on Camel’s Hump. We were definitely wrong about that.
We started from the Huntington side and followed the Burrows Trail on advice from a published guide. As we began our trudge, carrying our day packs full of water, extra layers of clothes, an assortment of trail foods, first aid material, and other articles, we were just a few minutes along and just getting used to the surface roots and rocks when we were passed by a single hiker carrying very little and moving along at a brisk pace. He said it was a beautiful day and a nice trail, and he wished us well and quickly disappeared into the distance. We trudged, as we always seem to do, considering the combined wisdom and discomfort of carrying so much weight up an irregular trail surface, slowly gaining elevation toward our distant goal. Would we get to the top today? Would we have to turn back? My heart thumped as we marched up the trail, and I had to stop frequently, not so much to catch my breath as to let the sound of my pounding heart subside.
Fitness is a relative thing. I am fit enough to tackle such hikes, and I appreciate the sense of accomplishment and the views when I reach the summit; but I am not fit enough to run, trot, or dance my way to the top. My wife and I move at a similar pace, and we both welcome the stops along the way. I don’t often admit it, but I appreciate her interest in stopping now and then for a snack on the trail.
As we labored on, we moved to the side of the trail several times to make way for several groups of young people and families who passed us on the way up. We looked for signs indicating our progress toward the summit, and we found there were not enough to be encouraging.
After what seemed like a half day of trudging, the Burrows Trail joined the Long Trail, and the trail steepened markedly, becoming an uneven series of giant stair steps of jagged rock and boulders, switch-backing in some places as we gained elevation.
“Yes,” I thought. “I am old. I was a fool to think this would be fun. These other hikers must wonder how I got up here and why I would try.” Surely, they imagined their elderly parents or grandparents at home in the rocker or in front of the TV as they came upon us and passed us. They were friendly and sometimes giggly as they patiently waited while we found a good place to step to the side of the trail. I was actually quite pleased when one group was going slowly to accommodate a member who was having noticeable difficulty with the exertion. “Aha!” I thought. “I am not alone. Even young people can be out of shape. Perhaps I will reach the summit ahead of her.” I soon forgot her, though, as conquering the giant steps consumed all of my attention.
The last section of the trail to the summit was more challenging as the rocks grew larger and the trail more treacherous with opportunities to step off into bottomless space. After a near mishap back-fall, we reached the summit and joined a dispersed crowd of hikers, dressed mostly in short sleeves, relaxing on the rocks, chatting, and a few playing with dogs. The dogs were curious but mostly well behaved. A young park ranger moved around the summit, asking hikers about their experience on the trail and at the summit, where they were from and going, and their planned route of descent. I asked her about taking the trail down the south side – was it passable from the top? (It did not appear to be.) She pointed toward a descent that would begin to the north side, wrap around the west side below the summit, and then continue south. It sounded easy enough.
As we started down and found that our steps had to be longer and that we had to rely more on lengthened trekking poles for balance as our feet reached out to land on surfaces that seemed too far away or too far down, I remembered how downhill hiking is often more strenuous than uphill hiking. As I had approached the summit earlier, I had felt a sense of relief that the hardest part of the day’s journey was behind me. Now, as we started down, I realized that going up had been the easiest part, despite the exertion and my pounding heart. Fear of falling had become my greatest challenge for the descent. Every step seemed too long, the landing place too far, the opportunity for mishap too great. We labored on but with a new kind of labor, stopping for breathtaking views and to find the courage to take the next step or few steps along a rock ledge or around a boulder that appeared to project into space. Only the sight or sound of oncoming people assured us that it really was a trail to somewhere other than air.

Rounding the bend, looking down south

The trail (Long Trail South) seemed to go on forever, challenging us to find its blazes across confusing rock outcroppings, down through rock ravines, and between giant slices of ledge that framed pinched spaces we had to traverse sideways or bent over backward like limbo dancers. “I am not this flexible,” I thought. “My joints need daily pills just to sit down, stand up from a chair, walk to the kitchen and open the refrigerator. These cannot be my bones and joints going through these gyrations and twists and turns to get down from this mountain. I should have waited just a few more years and be satisfied to have seen Camel’s Hump only from a distance. But, it’s too late now. I have to make it down from this mountain.”
We usually talk when the going is fun on the trail, even when we are feeling over-exerted on the way up. We did not talk on the way down this trail. We were each consumed with how to make the next move or series of moves. More than once, we had to backtrack when the apparent route turned out to be too difficult and we had to find an alternative. We went up around trees when the route looked inviting, but found ourselves looking down over cliffs.
It seemed as though we had descended thousands of feet and the sun had set several times before we finally reached the junction with the last leg of our loop – the Forest City Trail. It looked so easy and friendly that we thought we should be able to scamper along it like chipmunks as we envisioned our waiting car in the parking lot. But it was too late. We were too tired, shaken by the stress of the descent, no longer in full control of our extremities, which twitched and ached as we began to be bothered by the weight of our day packs, even though most of the water had been consumed. As we neared the end of the Forest City Trail and thought we would have only a few steps to the parking lot, we turned onto the Connector and discovered, much to our madness, that we had to climb the Connector to a higher elevation to reach the parking lot.
Then it was over. We were back, returning conquerors of Camel’s Hump. There was no one else to tell about it. Anyone we know who also knew the trail had done it quickly and more easily and maybe more than once, or they were people who would not even think of spending a day trudging up a trail and then suffering through such a compromising descent. We talked about it ourselves over dinner and then kept returning to the topic for several days. We swore we would never go there again.
But, who knows, maybe later this year we will do the same loop in reverse. After all, we are only a year older.
